 Introduction
Introduction
Knee arthroscopy is one of the most commonly used techniques in orthopaedics. It allows many injuries to be diagnosed and treated through two small incisions, causing less pain and enabling a quicker recovery than traditional open surgery. In this article, I’ll explain, in simple terms, how this technique has evolved, how it’s performed today, and in which cases it can help you.
 1. From large incisions to a tiny camera
1. From large incisions to a tiny camera
Not so long ago, knee surgery meant cutting the knee open completely to see what was going on inside. This resulted in large scars, more pain and very long recovery times.
In the early 20th century, the first attempts were made to ‘look inside’ joints using rigid instruments and with very limited visibility. It was not until the 1970s and 1980s that arthroscopy really began to develop, thanks to smaller cameras, cold light and improved irrigation systems.
The real breakthrough came with the introduction of fibre optics and high-definition cameras. Suddenly, we were able to see inside the knee with remarkable clarity and work with fine instruments without having to open up the joint.
Today, arthroscopy is an indispensable tool in orthopaedics: it is safe, precise and allows for a much quicker recovery for the patient.
 2. How arthroscopy is performed today
2. How arthroscopy is performed today
The technique is much simpler than many patients imagine:
Preparation
The patient enters the operating theatre under anaesthesia (general or regional, as appropriate). The leg is cleaned and positioned comfortably for the procedure.Two small incisions
Two small ‘windows’ measuring a few millimetres are made:- One for inserting the camera, usually the anterolateral portal
- Another one for the instruments: anteromedial portal
- Occasionally, additional access points are created as required by the surgical procedure.
Internal view
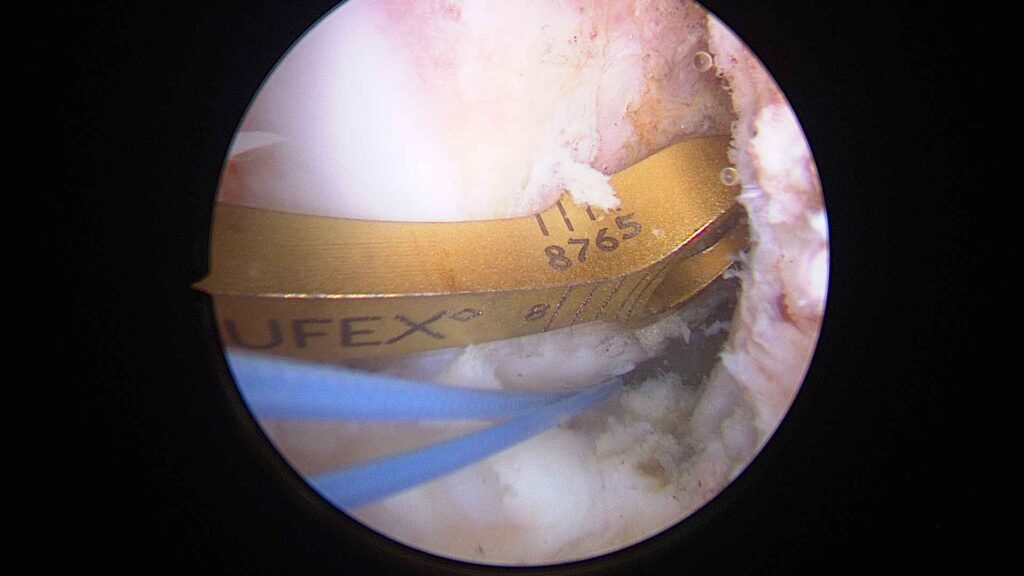
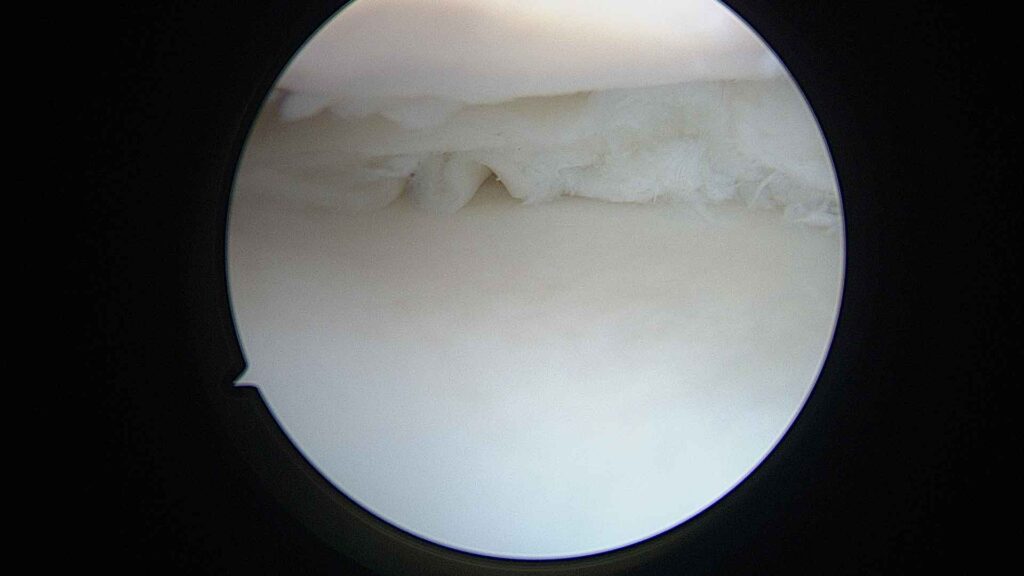
The camera transmits high-definition images to a monitor. This allows menisci, cartilage, ligaments and synovial tissue to be viewed in great detail.Treatment of the injury
Depending on the problem, specific instruments are used to repair, clean or remove the necessary tissue, such as the synoviotome, vaporiser, meniscal trimming forceps, fragment removal forceps, cartilage debridement punches, trephines to stimulate biological repair, and bone drilling bits, amongst others.Duration and discharge
The procedure usually lasts between 20 and 45 minutes. Patients are usually discharged on the same day; it is typically performed as a day-case procedure.




 3. What is arthroscopy actually used for?
3. What is arthroscopy actually used for?
Arthroscopy isn’t a ‘one-size-fits-all’ solution, but it is very useful for specific problems. Among the most common are:
Menisci
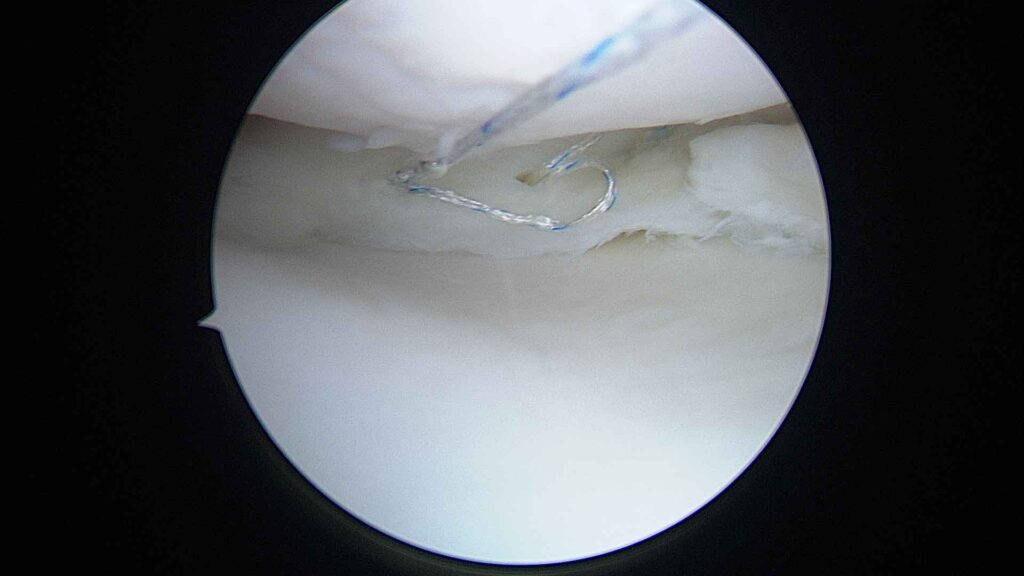
- Suturing tears.
- Rectification where the damage is irreparable.
- Treatment of meniscal tears
Cartilage
- Removal of loose debris.
- Cartilage stimulation techniques (microperforations).
- Filling osteochondral defects using gels, matrices, grafts, and other methods.
Synovitis
- Removal of inflamed tissue that causes pain or fluid build-up.
Free bodies
- Removal of fragments that move within the joint and cause blockages.
Intra-articular ligaments
- Arthroscopy forms part of the reconstruction technique for the ACL, the most commonly injured ligament, involving the use of small incisions to harvest the graft and secure it in place using screws, staples or cortical suspension.
 4. When it is recommended… and when it is not
4. When it is recommended… and when it is not
 Recommended for:
Recommended for:
- There is a clear locking of the knee.
- There is a meniscal tear causing mechanical pain.
- There are loose bodies within the joint.
- A cartilage injury needs to be treated.
- It is part of ACL surgery.
✘ Not recommended when:
There is advanced osteoarthritis (arthroscopy does not “cure” osteoarthritis).
- The pain is diffuse and there is no obvious mechanical problem.
- The MRI scan does not show any treatable lesion.
In everyday terms, arthroscopy is useful when the knee locks up, fails to rotate, swells repeatedly or causes mechanical pain. An important point to note: surgery is not always the best option. A clinical examination and an MRI scan help to make an accurate decision.
 5. What to expect after arthroscopy
5. What to expect after arthroscopy
Recovery is usually quick, but it’s worth knowing what’s normal:
Mild to moderate pain during the first few days.
Foot support is almost always provided from day one, except in specific cases.
Back to work:
- Offices: 10–15 days.
- Physical work: 4–6 weeks.
Sport: it depends on the injury being treated, but it usually takes between 4 and 12 weeks.
Physiotherapy: started early, it is essential for regaining strength and mobility.
Warning signs:
- Fever.
- A significant increase in pain.
- Excessive swelling.
- Redness around the incisions.
- Severe bruising
- Chest pain or difficulty breathing
 6. Practical advice following surgery
6. Practical advice following surgery
Ice: 15–20 minutes, several times a day, always with protection.
Medicines: painkillers, anti-inflammatories and prescribed anticoagulants.
Stairs: go up using your good leg, go down using the one that’s been operated on.
Gentle exercises: ankle mobility, straight-leg raises, quadriceps contractions. Ensure the knee is fully extended and return to flexion in accordance with post-operative guidelines.
Footwear: comfortable, stable and well-cushioned.
Avoid: walking too soon, carrying unnecessary weight, deep squats.
 7. Myths and realities
7. Myths and realities
“Arthroscopy fixes everything”
No. It’s very useful, but it’s not effective for treating advanced osteoarthritis.
“It’s a minor operation, so there’s no need to take care of yourself afterwards”
You do need to. Recovery depends heavily on post-operative care.
“If I have the operation, I won’t have any more pain”
It depends on the source of the pain. If the cause is mechanical, it improves. If it’s osteoarthritis, not always.
“Recovery is immediate”
It’s quick, but not instant. Physiotherapy is key.
Conclusion
Knee arthroscopy is a safe, effective and widely used technique that has revolutionised the treatment of many injuries. It allows the inside of the joint to be viewed and repaired through tiny incisions, with a much quicker recovery than traditional surgery. However, it is not the solution for all knee problems, and each case must be assessed individually.